Κόμβος Μάθησης
Ανακαλύψτε πηγές που θα σας βοηθήσουν να κατανοήσετε και να διαχειριστείτε την ψωριασική αρθρίτιδα.
Εγχειρίδιο Ψωριασικής Αρθρίτιδας
Διαχείριση Ψωριασικής Αρθρίτιδας: Θεραπείες και Τρόπος Ζωής
Πώς αντιμετωπίζεται η ψωριασική αρθρίτιδα?
Αν και δεν υπάρχει θεραπεία για την ψωριασική αρθρίτιδα, υπάρχουν πολλαπλές φαρμακευτικές θεραπευτικές επιλογές που λειτουργούν για τον έλεγχο της νόσου και των συμπτωμάτων της (3). Οι φαρμακευτικές θεραπείες ειδικά για την ψωριασική αρθρίτιδα επικεντρώνονται σε:
ΘΕΡΑΠΕΊΕΣ ΜΕ ΦΆΡΜΑΚΑ

-
επιβράδυνση της εξέλιξης της πάθησης;
-
μείωση της φλεγμονής;
-
ανακούφιση από τον πόνο;
-
αντιμετώπιση δερματικών συμπτωμάτων;
-
διατήρηση των αρθρώσεων όσο το δυνατόν πιο κινητικές.
Για τους περισσότερους ανθρώπους, η θεραπεία της ψωριασικής αρθρίτιδας περιλαμβάνει τη δοκιμή πολλών διαφορετικών φαρμάκων. Δεδομένου ότι πολλοί άνθρωποι με ψωριασική αρθρίτιδα έχουν και ψωρίαση, η διαχείριση της πάθησης πιθανόν να αφορά τη θεραπεία δύο ασθενειών. Ορισμένες θεραπείες δρουν και στις δύο ασθένειες, ενώ άλλες δρουν κυρίως στην αρθρίτιδα ή στα δερματικά προβλήματα.
Κάθε άτομο που διαγιγνώσκεται με ψωριασική αρθρίτιδα είναι διαφορετικό. Οι γιατροί συνιστούν ορισμένες θεραπείες ανάλογα με:
-
πόσα και ποια μέρη του σώματος επηρεάζονται;
-
πόσο σοβαρή είναι η ασθένεια;
-
φαρμακευτικές αλλεργίες και άλλες καταστάσεις υγείας;
-
τρέχουσα χρήση φαρμάκων.
Πολλές φορές, τα άτομα με ψωριασική αρθρίτιδα μπορεί να χρειαστεί να λάβουν ταυτόχρονα περισσότερα από ένα φάρμακα για τον έλεγχο της νόσου - αυτό ονομάζεται συνδυαστική θεραπεία. Η συνδυαστική θεραπεία μπορεί να επιτρέψει τη χρήση χαμηλότερων δόσεων κάθε μεμονωμένου φαρμάκου.
Κατά τη διάρκεια των εξάρσεων, μπορεί να προστεθούν προσωρινά ή μακροπρόθεσμα πρόσθετα φάρμακα
Είναι σημαντικό να συμμετέχετε στη λήψη αποφάσεων από κοινού με τον/τους γιατρό/ους σας και να τηρείτε το θεραπευτικό πρόγραμμα. Θα πρέπει να γνωστοποιείτε τυχόν προβλήματα με τα φάρμακα, όπως παρενέργειες ή δυσκολία στην τήρηση του σχεδίου θεραπείας, ώστε να μπορούν να ληφθούν αποτελεσματικά μέτρα για την αντιμετώπιση του προβλήματος (των προβλημάτων).
ΘΕΡΑΠΕΊΑ ΓΙΑ ΤΗΝ ΑΡΘΡΊΤΙΔΑ
Τα μη συνταγογραφούμενα και συνταγογραφούμενα φάρμακα για την ψωριασική αρθρίτιδα περιλαμβάνουν:
-
Μη στεροειδή αντιφλεγμονώδη φάρμακα (ΜΣΑΦ),
-
Στεροειδή φάρμακα (κορτικοστεροειδή),
-
Τροποποιητικά της νόσου αντιρευματικά φάρμακα (DMARDs).



Μη στεροειδή αντιφλεγμονώδη φάρμακα (ΜΣΑΦ)
Τα ΜΣΑΦ μπορούν να βοηθήσουν στην ανακούφιση του πόνου και στη μείωση της φλεγμονής, αλλά μπορεί να μην είναι αρκετά για την αντιμετώπιση των συμπτωμάτων της ψωριασικής αρθρίτιδας (9).
Υπάρχουν δύο τύποι ΜΣΑΦ:
-
παραδοσιακά ΜΣΑΦ, όπως η ιβουπροφαίνη, η ναπροξένη και η δικλοφενάκη, και,
-
Αναστολείς COX-2, όπως η σελεκοξίμπη και η ετορικοξίμπη.
Όπως όλα τα φάρμακα, έτσι και τα ΜΣΑΦ μπορεί να έχουν παρενέργειες. Ο γιατρός σας θα λάβει προφυλάξεις για να μειώσει τον κίνδυνο παρενεργειών, συνταγογραφώντας τη χαμηλότερη δόση που είναι απαραίτητη για τον έλεγχο των συμπτωμάτων σας για το συντομότερο δυνατό χρονικό διάστημα.
Τα ΜΣΑΦ μπορούν μερικές φορές να επηρεάσουν το στομάχι και το έντερο, προκαλώντας πεπτικά προβλήματα, όπως δυσπεψία και έλκος στομάχου (17). Ένα φάρμακο που ονομάζεται αναστολέας αντλίας πρωτονίων (PPI), όπως η ομεπραζόλη ή η λανσοπραζόλη, μπορεί επίσης να συνταγογραφηθεί για να βοηθήσει στην προστασία του στομάχου.
Η χρόνια θεραπεία με ΜΣΑΦ μπορεί επίσης να αυξήσει τον κίνδυνο καρδιακών προσβολών, εγκεφαλικών επεισοδίων και άλλων καρδιακών προβλημάτων (17). Παρακαλούμε, ενημερώστε τον γιατρό σας εάν υπάρχουν παράγοντες κινδύνου που μπορεί να αυξήσουν τον συνολικό σας κίνδυνο, για παράδειγμα κάπνισμα, υψηλή αρτηριακή πίεση, υψηλή χοληστερόλη, διαβήτης ή οικογενειακό ιστορικό καρδιακής νόσου. Ορισμένοι άνθρωποι διαπίστωσαν ότι η λήψη ΜΣΑΦ επιδείνωσε τα συμπτώματα της ψωρίασης. Ενημερώστε το γιατρό σας εάν σας συμβεί αυτό.
Στεροειδή φάρμακα (κορτικοστεροειδή)
Όπως και τα ΜΣΑΦ, τα κορτικοστεροειδή μπορούν να βοηθήσουν στη μείωση της φλεγμονής και του πόνου (18).
Εάν έχετε μία μόνο επώδυνη ή/και πρησμένη άρθρωση, ο γιατρός σας μπορεί να χορηγήσει το φάρμακο απευθείας στην άρθρωση. Το αποτέλεσμα μπορεί να διαρκέσει από μερικές εβδομάδες έως αρκετούς μήνες. Ωστόσο, οι πάρα πολλές ενέσεις στεροειδών στην ίδια άρθρωση (ή στις ίδιες αρθρώσεις) μπορεί να βλάψουν τον περιβάλλοντα ιστό και, επομένως, ο γιατρός σας συνήθως δεν συνιστά περισσότερες από τρεις ενέσεις ετησίως.
Όταν πολλές αρθρώσεις είναι φλεγμονώδεις, τα κορτικοστεροειδή μπορούν να ληφθούν ως δισκία ή ως ένεση στον μυ. Ωστόσο, οι γιατροί είναι επιφυλακτικοί ως προς αυτό, επειδή τα κορτικοστεροειδή μπορεί να προκαλέσουν παρενέργειες, όπως αύξηση του σωματικού βάρους και οστεοπόρωση, αυξημένο κίνδυνο λοιμώξεων και καρδιαγγειακών επεισοδίων, εάν χρησιμοποιούνται για μεγάλα χρονικά διαστήματα. Λόγω αυτών των παρενεργειών, ο γιατρός σας θα σας συνταγογραφήσει τη χαμηλότερη δόση που είναι απαραίτητη για τον έλεγχο των συμπτωμάτων σας για το συντομότερο δυνατό χρονικό διάστημα. Η ψωρίαση μπορεί να αναζωπυρωθεί όταν σταματήσετε τη χρήση κορτικοστεροειδών από το στόμα.
Τροποποιητικά της νόσου αντιρρευματικά φάρμακα (DMARDs)
Τα DMARDs είναι ισχυρά φάρμακα που μειώνουν τη φλεγμονή και μπορούν να σταματήσουν την επιδείνωση της ψωριασικής αρθρίτιδας (19). Τα DMARDs μπορούν να βοηθήσουν στην πρόληψη της βλάβης στις αρθρώσεις σας.
Πολλά DMARD αντιμετωπίζουν τόσο την ψωρίαση όσο και την ψωριασική αρθρίτιδα. Επειδή αυτός ο τύπος φαρμάκου αντιμετωπίζει την αιτία της πάθησής σας και όχι τα συμπτώματα, μπορεί να χρειαστούν έως και τρεις μήνες προτού αισθανθείτε αποτέλεσμα. Ως εκ τούτου, είναι σημαντικό να συνεχίσετε να παίρνετε το φάρμακο, ακόμη και αν στην αρχή δεν φαίνεται να λειτουργεί.
Όπως όλα τα φάρμακα, έτσι και τα DMARDs μπορεί να έχουν ορισμένες παρενέργειες. Ενώ τα DMARDs μπορεί να είναι πολύ αποτελεσματικά, τα φάρμακα αυτά μειώνουν τη δραστηριότητα του ανοσοποιητικού συστήματος (ανοσοκατασταλτικά) και αυξάνουν τον κίνδυνο λοίμωξης. Ωστόσο, είναι σημαντικό να θυμάστε ότι η μη θεραπεία της ψωριασικής αρθρίτιδας μπορεί να οδηγήσει σε μόνιμη βλάβη των οστών και των αρθρώσεων.
Υπάρχουν τρεις τύποι DMARDs όπως περιγράφονται στον Πίνακα 1.
Πίνακα 1: Τύποι τροποποιητικών της νόσου αντιρρευματικών φαρμάκων.
Συμβατικό
Τα συμβατικά DMARDs (csDMARDs) έχουν χρησιμοποιηθεί για μεγαλύτερο χρονικό διάστημα και έχουν ευρεία ανοσοκατασταλτική δράση. Αυτά τα φάρμακα λαμβάνονται συνήθως από το στόμα.
Παράδειγμα: μεθοτρεξάτη, σουλφασαλαζίνη.
Βιολογικό
Τα βιολογικά DMARDs (bDMARDs) διακόπτουν βασικά στάδια της φλεγμονώδους διαδικασίας και γενικά δρουν ταχύτερα από τα παραδοσιακά DMARDs. Αυτά τα φάρμακα χορηγούνται συνήθως με ένεση.
Παράδειγμα: αδαλιμουμάμπη, ετανερσέπτη.
Στοχευμένο συνθετικό
Όπως και τα βιολογικά DMARDs, τα συνθετικά DMARDs (tsDMARDs) εμποδίζουν βασικά στάδια της φλεγμονώδους διαδικασίας. Αυτά τα φάρμακα λαμβάνονται συνήθως από το στόμα.
Παράδειγμα: τοφασιτινίμπη.
ΘΕΡΑΠΕΊΑ ΓΙΑ ΤΗΝ ΨΩΡΊΑΣΗ
Τα μη συνταγογραφούμενα και συνταγογραφούμενα φάρμακα για την ψωρίαση περιλαμβάνουν:
-
τοπικά φάρμακα από βιταμίνη D, παράγωγα της βιταμίνης Α, σαλικυλικό οξύ, πίσσα άνθρακα ή κορτικοστεροειδή,
-
η φωτοθεραπεία που χρησιμοποιεί υπεριώδες φως (UVB) μπορεί να συνταγογραφηθεί για τη θεραπεία και τη μείωση των δερματικών εξανθημάτων. Μόνο ο γιατρός σας θα πρέπει να σας συνταγογραφήσει φωτοθεραπεία, μην προσπαθήσετε να χρησιμοποιήσετε το ηλιακό φως ή τους ηλιακούς λαμπτήρες για να θεραπεύσετε μόνοι σας το δέρμα σας,
-
ορισμένα DMARDs και βιολογικές θεραπείες που χρησιμοποιούνται για την αρθρίτιδα μπορούν επίσης να βοηθήσουν την ψωρίαση.

ΕΜΒΌΛΙΑ
Εάν έχετε ψωριασική αρθρίτιδα, μπορεί να έχετε υψηλότερο κίνδυνο λοίμωξης και οι λοιμώξεις μπορεί να είναι πιο σοβαρές (20). Αυτό μπορεί να οφείλεται στην ίδια την αρθρίτιδα ή στη θεραπεία της.
Η ψωριασική αρθρίτιδα, η οποία προκαλείται από βλάβη του ανοσοποιητικού συστήματος, μπορεί να σας κάνει πιο ευάλωτους στις λοιμώξεις. Επιπλέον, ορισμένα από τα φάρμακα που χρησιμοποιούνται για τη θεραπεία της ψωριασικής αρθρίτιδας (π.χ., DMARDs ή/και στεροειδή) εξασθενούν το ανοσοποιητικό σύστημα, δηλαδή δρουν ως ανοσοκατασταλτικά, γεγονός που μπορεί επίσης να σας κάνει πιο επιρρεπείς σε λοιμώξεις.
Ο αυξημένος κίνδυνος λοίμωξης λόγω ιατρικής κατάστασης ή/και φαρμάκων ονομάζεται ανοσοκαταστολή.
Ο ρευματολόγος σας μπορεί να παράσχει καθοδήγηση με βάση την ηλικία σας και τον κίνδυνο να προσβληθείτε από ορισμένα λοιμώδη νοσήματα (π.χ., COVID-19, γρίπη, πνευμονία, έρπητα ζωστήρα ή ηπατίτιδα Β). Τα εμβόλια είναι ασφαλή και μπορούν να σας βοηθήσουν να αποφύγετε σοβαρές λοιμώξεις.

ΜΗ ΦΑΡΜΑΚΟΛΟΓΙΚΈΣ ΘΕΡΑΠΕΊΕΣ
Τα φάρμακα δεν είναι ο μόνος τρόπος για τη θεραπεία ή τη διαχείριση των συμπτωμάτων της ψωριασικής αρθρίτιδας. Υπάρχουν πολλά πράγματα που μπορείτε να κάνετε, παράλληλα με τη λήψη συνταγογραφούμενων φαρμάκων, τα οποία μπορούν να βελτιώσουν την ποιότητα της ζωής σας μειώνοντας τον πόνο και τη φλεγμονή και βελτιώνοντας τη γενική σας υγεία.
Η ΦΩΝΉ ΣΑΣ ΈΧΕΙ ΣΗΜΑΣΊΑ
Οι εμπειρίες σας - πώς λειτουργούν οι θεραπείες σας, ποιες παρενέργειες αντιμετωπίζετε, πώς σας επηρεάζουν τα συμπτώματά σας, ποιες προκλήσεις αντιμετωπίζετε στην καθημερινή σας ζωή λόγω της ψωριασικής αρθρίτιδας - είναι πολύ σημαντικές πληροφορίες.
Αυτές οι πληροφορίες ονομάζονται αποτελέσματα που αναφέρουν οι ασθενείς (PROs) και μπορεί να συλλέγονται μέσω ερωτηματολογίου πριν από το ρευματολογικό σας ραντεβού. Τα PROs μπορούν να βοηθήσουν τον γιατρό σας να εκτιμήσει τις επιπτώσεις της νόσου σας και να αξιολογήσει καλύτερα το θεραπευτικό σας πλάνο. Αυτά τα ερωτηματολόγια μπορούν επίσης να σας βοηθήσουν στην αυτοδιαχείριση της κατάστασής σας.
Μερικά από τα ερωτηματολόγια που μπορεί να χρησιμοποιήσει ο ρευματολόγος σας είναι:
-
PSAID (Ψωριασική Αρθρίτιδα Επίδραση της Νόσου): μετρά τον αντίκτυπο της νόσου σας στη σωματική και ψυχολογική σας υγεία,
-
VAS (Οπτική Αναλογική Κλίμακα): ένα απλό εργαλείο για την παρακολούθηση και τη μέτρηση του πόνου σας,
-
IPAQ (Διεθνές Ερωτηματολόγιο Φυσικής Δραστηριότητας): μετράει τους τύπους έντασης της φυσικής δραστηριότητας και του χρόνου που κάθονται οι άνθρωποι στο πλαίσιο της καθημερινής τους ζωής,
-
HAQ (Ερωτηματολόγιο Αξιολόγησης Υγείας): μετρά τη φυσική σας λειτουργία και την αναπηρία λόγω αρθρίτιδας,
-
FACIT-F (Λειτουργική Εκτίμηση Θεραπείας Χρόνιας Νόσου – Κόπωσης): μετρά την κόπωση που σας προκαλεί η αρθρίτιδα,
-
WPAI (Παραγωγικότητα Εργασίας και Απομείωση Δραστηριότητας): μετρά τις βλάβες στην εργασία και τις δραστηριότητες,
-
HADS (Νοσοκομειακή κλίμακα άγχους και κατάθλιψης): μετρά τα επίπεδα άγχους και κατάθλιψης,
-
PsAQoL (Ψωριασική Αρθρίτιδα Ποιότητα Ζωής): μετρά την ποιότητα ζωής σε άτομα με ψωριασική αρθρίτιδα,
-
EQ-5D (EuroQol-5 Διαστάσεις): μετρά την ποιότητα ζωής σε σχέση με 5 διαστάσεις - κινητικότητα, συνήθεις δραστηριότητες, αυτοεξυπηρέτηση, πόνος και δυσφορία, άγχος και κατάθλιψη,
-
SF-36 (Σύντομη Φόρμα-36): μετρά την ποιότητα ζωής και καλύπτει 8 τομείς της υγείας - σωματική λειτουργικότητα, σωματικό ρόλο, πόνο, γενική υγεία, ζωτικότητα, κοινωνική λειτουργία, συναισθηματικό ρόλο και ψυχική υγεία.
Έτσι, αν ο γιατρός ή ο νοσηλευτής σας, σας ζητήσει να συμπληρώσετε ένα ερωτηματολόγιο, παρακαλούμε αφιερώστε χρόνο για να το κάνετε και να είστε ειλικρινείς!
ΦΥΣΙΚΟΘΕΡΑΠΕΊΑ ΚΑΙ ΕΡΓΟΘΕΡΑΠΕΊΑ
Η φλεγμονή των αρθρώσεων και των μαλακών μορίων μπορεί συχνά να οδηγήσει σε ακραίο πόνο, ακινησία και δυσλειτουργία. Επιπλέον, η αρθρίτιδα μπορεί να οδηγήσει σε δυσκολία στις καθημερινές δραστηριότητες στο σπίτι και στο χώρο εργασίας. Η φυσικοθεραπεία και η εργοθεραπεία μπορούν να σας βοηθήσουν να κινηθείτε με ασφάλεια και αποτελεσματικότητα.
Η φυσικοθεραπεία είναι η πιο αποτελεσματική εάν αντιμετωπίζετε (21):
-
απώλεια κίνησης λόγω φλεγμονής στον ώμο, τον καρπό, το χέρι, το γόνατο ή το πόδι,
-
σοβαρή ενθεσίτιδα ή δακτυλίτιδα,
-
φλεγμονώδης πόνος στην πλάτη.
Η φυσικοθεραπεία θα επικεντρωθεί σε (21):
-
βελτίωση της κινητικότητας και αποκατάσταση της χρήσης των προσβεβλημένων αρθρώσεων,
-
αύξηση της μυϊκής δύναμης για τη στήριξη των αρθρώσεων,
-
διατήρηση της φυσικής κατάστασης,
-
διατήρηση της ικανότητας εκτέλεσης καθημερινών δραστηριοτήτων.
Η εργοθεραπεία μπορεί επίσης να είναι χρήσιμη, ειδικά αν αντιμετωπίζετε δυσκολίες με τις καθημερινές δραστηριότητες.

Η εργοθεραπεία μπορεί να σας βοηθήσει να μεγιστοποιήσετε την ικανότητά σας να συμμετέχετε στις καθημερινές δραστηριότητες.
Οι στρατηγικές περιλαμβάνουν τη χρήση βοηθητικών συσκευών (π.χ., υποστηρικτικούς νάρθηκες) και την τροποποίηση της κίνησης για να βοηθηθούν οι άνθρωποι να προστατεύσουν τις αρθρώσεις τους, εκτελώντας εργασίες με διαφορετικούς τρόπους από ό,τι έχουν συνηθίσει (π.χ., χρησιμοποιώντας και τα δύο χέρια).

ΧΕΙΡΟΥΡΓΙΚΉ ΕΠΈΜΒΑΣΗ
Τα περισσότερα άτομα που διαγιγνώσκονται με ψωριασική αρθρίτιδα δεν θα χρειαστούν ποτέ χειρουργική επέμβαση στις αρθρώσεις. Ωστόσο, εάν οι αρθρώσεις έχουν υποστεί σοβαρή βλάβη από την αρθρίτιδα ή εάν άλλες θεραπείες δεν μειώνουν τον πόνο, οι κατεστραμμένες αρθρώσεις μπορούν να αντικατασταθούν από πλαστικές, μεταλλικές ή κεραμικές προθέσεις για τη μείωση του πόνου και τη βελτίωση της λειτουργίας και της ποιότητας ζωής.
ΕΝΑΛΛΑΚΤΙΚΕΣ ΘΕΡΑΠΕΙΕΣ
Ορισμένα άτομα με ψωριασική αρθρίτιδα θεωρούν ότι οι εναλλακτικές θεραπείες μπορεί να είναι χρήσιμες. Ωστόσο, θα πρέπει πάντα να συζητάτε με το γιατρό σας πριν δοκιμάσετε οι εναλλακτικές θεραπείες.
Δεν υπάρχουν επιστημονικά στοιχεία που να υποστηρίζουν ότι η λήψη οποιουδήποτε είδους συμπληρώματος διατροφής, όπως οι κάψουλες ιχθυελαίου, λειτουργεί στη θεραπεία της ψωριασικής αρθρίτιδας.
Επιπλέον, δεν υπάρχουν αρκετά επιστημονικά στοιχεία για να υποστηριχθεί η χρήση εναλλακτικών θεραπειών, όπως η λουτροθεραπεία ή ο βελονισμός, ως θεραπείες για την ψωριασική αρθρίτιδα.
Οι εναλλακτικές θεραπείες μπορεί να αντιδράσουν με άλλες θεραπείες, για αυτό θα πρέπει να μιλήσετε με το γιατρό σας εάν χρησιμοποιείτε ή σκέφτεστε να χρησιμοποιήσετε κάποια από αυτές.
ΑΥΤΟΦΡΟΝΤΊΔΑ ΚΑΙ ΤΡΌΠΟΣ ΖΩΉΣ

Καθιστική συμπεριφορά
Η καθιστική συμπεριφορά, η οποία χαρακτηρίζεται από παρατεταμένες περιόδους καθίσματος, όταν συσσωρεύεται καθημερινά για περισσότερες από 8 ώρες ή διατηρείται για διάστημα μεγαλύτερο των 30 λεπτών χωρίς διακοπή, αποτελεί κίνδυνο για την υγεία και την ευημερία.
Τα άτομα που ζουν με ψωριασική αρθρίτιδα θα πρέπει να υιοθετήσουν μια προσαρμοσμένη ρουτίνα σωματικής δραστηριότητας, λαμβάνοντας υπόψη τα συγκεκριμένα συμπτώματα και τους περιορισμούς τους. Δεδομένου ότι η μηχανική καταπόνηση σε περίπτωση φλεγμονώδους κρίσης μπορεί να προωθήσει την εμφάνιση ενθεσίτιδας, είναι απαραίτητο να ελεγχθεί η φλεγμονή πριν από την αύξηση του επιπέδου της συνήθους σωματικής δραστηριότητας ή την έναρξη ενός προγράμματος άσκησης. Σε κάθε περίπτωση, οι ευεργετικές επιδράσεις της σωματικής δραστηριότητας και της άσκησης στη νόσο, την ευεξία και τις συναφείς συννοσηρότητες υπερτερούν του κινδύνου ενθεσίτιδας που προκαλείται από μηχανική καταπόνηση, ο οποίος είναι χαμηλός (25).
Διατροφή
Παρόλο που δεν υπάρχει συγκεκριμένη δίαιτα που μπορεί να θεραπεύσει την ψωριασική αρθρίτιδα, η υιοθέτηση ενός θρεπτικού και ισορροπημένου διατροφικού προγράμματος μπορεί να διαδραματίσει ζωτικό ρόλο στη διαχείριση των συμπτωμάτων και στη βελτίωση της συνολικής ευεξίας.
Οι έρευνες δείχνουν ότι η υιοθέτηση μιας μεσογειακού τύπου διατροφής (Εικόνα 3, αριστερή πλευρά), η οποία περιλαμβάνει φρούτα, λαχανικά, φυτικές ίνες, υψηλής ποιότητας λιπαρά και βιταμίνες, μπορεί να μειώσει τις επιπτώσεις της ψωριασικής αρθρίτιδας (26). Αυτός ο τύπος διατροφής έχει αντιφλεγμονώδη οφέλη που βοηθούν στη διαχείριση της δραστηριότητας της νόσου. Έτσι, δοκιμάζοντας αυτή τη διατροφική προσέγγιση μπορεί να σας βοηθήσει να απαλύνετε τα συμπτώματα της ψωριασικής αρθρίτιδας.
Η ενσωμάτωση ωμέγα-3 λιπαρών οξέων, που συνήθως βρίσκονται στα λιπαρά ψάρια (όπως ο σολομός, το σκουμπρί ή ο λιναρόσπορος), μπορεί επίσης να έχει αντιφλεγμονώδη αποτελέσματα, μειώνοντας ενδεχομένως τη δυσκαμψία και την ευαισθησία των αρθρώσεων (27).
Τα αντιοξειδωτικά που βρίσκονται στα πολύχρωμα φρούτα και λαχανικά (όπως τα μούρα, το σπανάκι και το λάχανο) προσφέρουν επίσης ισχυρές αντιφλεγμονώδεις ιδιότητες που θα μπορούσαν να ανακουφίσουν τη φλεγμονή των αρθρώσεων και τη δυσφορία των ατόμων που πάσχουν από ψωριασική αρθρίτιδα.

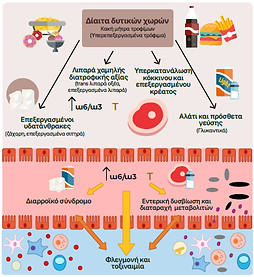
Εικόνα 3: Ωφέλιμα (στην αριστερή πλευρά) και επιβλαβή (στη δεξιά πλευρά) διατροφικά πρότυπα. Προσαρμογή από Guilliams et al., 2023 (28).
Συνολικά, συνιστάται να στοχεύετε σε μια ισορροπημένη πρόσληψη 2-5 μερίδων φρούτων και 3-5 μερίδων λαχανικών καθημερινά, καθώς αυτά τα πλούσια σε θρεπτικά συστατικά τρόφιμα παρέχουν απαραίτητα αντιοξειδωτικά που μπορούν να συμβάλουν στη διαχείριση της φλεγμονής των αρθρώσεων και της συνολικής υγείας.
Σε άτομα που ζουν με ψωριασική αρθρίτιδα, μελέτες υποδεικνύουν ότι η καθιστική συμπεριφορά μπορεί να συμβάλλει στην αυξημένη δυσκαμψία των αρθρώσεων, στη μειωμένη μυϊκή δύναμη και στη μειωμένη λειτουργία των αρθρώσεων. Επιπλέον, η καθιστική ζωή μπορεί να επιδεινώσει συμπτώματα, όπως η κόπωση και η κατάθλιψη, τα οποία είναι κοινά στην ψωριασική αρθρίτιδα. Αν και οι ακριβείς μηχανισμοί δεν είναι πλήρως κατανοητοί, η διατήρηση ενός ενεργού τρόπου ζωής θεωρείται γενικά ευεργετική για τη διαχείριση των συμπτωμάτων της ψωριασικής αρθρίτιδας.
Οι κίνδυνοι της καθιστικής συμπεριφοράς αυξάνονται ακόμη περισσότερο όταν οι άνθρωποι είναι αδρανείς, δηλαδή δεν συμμορφώνονται με τις συστάσεις του Παγκόσμιου Οργανισμού Υγείας (ΠΟΥ) για σωματική δραστηριότητα, οι οποίες περιγράφονται παρακάτω.
Σωματική δραστηριότητα
Η τακτική σωματική δραστηριότητα έχει αποδειχθεί ότι έχει πολλά οφέλη για τα άτομα που ζουν με ψωριασική αρθρίτιδα. Η σωματική δραστηριότητα αφορά όλες τις κινήσεις του σώματος που προκύπτουν από τη σύσπαση των μυών, ανεξάρτητα από το πλαίσιο στο οποίο πραγματοποιούνται, π.χ., αναψυχή, μεταφορά από και προς μέρη ή στο πλαίσιο της εργασίας ενός ατόμου.
Η σωματική δραστηριότητα μπορεί να συμβάλει στη βελτίωση της ευελιξίας των αρθρώσεων, στη μείωση της φλεγμονής και στην ενίσχυση της συνολικής λειτουργίας των αρθρώσεων. Επιπλέον, η σωματική δραστηριότητα μπορεί να συμβάλει στην καλύτερη ψυχική υγεία, καθώς μπορεί να βοηθήσει στην ανακούφιση των συμπτωμάτων κατάθλιψης και άγχους που συχνά συνδέονται με χρόνιες παθήσεις όπως η ψωριασική αρθρίτιδα. Η σωματική δραστηριότητα παίζει επίσης ρόλο στη διαχείριση του βάρους, η οποία είναι απαραίτητη, καθώς το υπερβολικό βάρος μπορεί να αυξήσει το στρες των αρθρώσεων (22).
Σύμφωνα με τον ΠΟΥ, συνιστάται η συλλογή τουλάχιστον ~20 λεπτών καθημερινής σωματικής δραστηριότητας, όπως το γρήγορο περπάτημα (23). Η σύσταση αυτή υιοθετείται επίσης από την Ευρωπαϊκή Συμμαχία Συλλόγων Ρευματολογίας (24).
Μια 20λεπτη σωματική δραστηριότητα μέτριας έντασης αντιστοιχεί σε συλλογή περίπου 2000 βημάτων. Λαμβάνοντας υπόψη μια λειτουργική δραστηριότητα 4500 βημάτων ανά ημέρα που συνδέεται με την εκτέλεση δραστηριοτήτων καθημερινής ζωής, όπως η περιποίηση, το μαγείρεμα, η καθαριότητα, η μετακίνηση από και προς την εργασία/σχολείο, οι συστάσεις του ΠΟΥ, όταν εκφράζονται σε συνολικό αριθμό βημάτων ανά ημέρα, αντιπροσωπεύουν το άθροισμα των δύο τύπων δραστηριότητας και αντιστοιχούν σε συλλογή 6500 καθημερινών βημάτων υπό κανονικές συνθήκες διαβίωσης.
Σωματική άσκηση
Οι πιο ωφέλιμοι τύποι άσκησης για την ψωριασική αρθρίτιδα επικεντρώνονται στη βελτίωση της ευελιξίας, της δύναμης και της καρδιαγγειακής κατάστασης χωρίς να προκαλούν υπερβολική καταπόνηση των αρθρώσεων. Συχνά συνιστώνται δραστηριότητες χαμηλής επιβάρυνσης, όπως το κολύμπι, το περπάτημα και η ποδηλασία. Οι ασκήσεις ενδυνάμωσης, συμπεριλαμβανομένης της άσκησης αντίστασης και της ήπιας γιόγκα, μπορούν να βοηθήσουν στην ενίσχυση της μυϊκής υποστήριξης γύρω από τις αρθρώσεις
Οι ασκήσεις με βάση το νερό είναι ιδιαίτερα επωφελείς, καθώς παρέχουν άνωση, μειώνοντας τις επιπτώσεις στις αρθρώσεις. Τα οφέλη αυτών των ασκήσεων περιλαμβάνουν αυξημένη κινητικότητα των αρθρώσεων, μειωμένο πόνο και δυσκαμψία, βελτιωμένο μυϊκό τόνο και καλύτερη συνολική ευεξία.
Η εφαρμογή iPROLEPSIS σκοπεύει να σας βοηθήσει να περιορίσετε τις καθιστικές συμπεριφορές, να αυξήσετε τη σωματική δραστηριότητα και να βελτιώσετε την καθημερινή λειτουργική ικανότητα με συγκεκριμένες και ασφαλείς συστάσεις προγραμμάτων προπόνησης (για περισσότερες πληροφορίες δείτε την ενότητα “iPROLEPSIS”).
Η μείωση της πρόσληψης ζάχαρης, κορεσμένων λιπαρών και νατρίου μπορεί να σας βοηθήσει να διατηρήσετε ένα υγιές βάρος. Η παχυσαρκία συνδέεται με υψηλότερες πιθανότητες εμφάνισης ψωριασικής αρθρίτιδας, υπογραμμίζοντας τη σημασία της διαχείρισης του βάρους, ειδικά για τους ασθενείς με ψωρίαση που συχνά πάσχουν από μεταβολικό σύνδρομο και παχυσαρκία (29).
Το υπερβολικό βάρος μπορεί να αυξήσει τη δυσφορία και τη φλεγμονή των αρθρώσεων, ιδίως στις αρθρώσεις που φέρουν φορτίο (όπως τα ισχία, τα γόνατα και η σπονδυλική στήλη). Συνεπώς, προσέξτε τις διατροφικές σας επιλογές, καθώς αυτές μπορούν να σας βοηθήσουν να διαχειριστείτε τα συμπτώματά σας.
Η βιταμίνη D βοηθά στην απορρόφηση του ασβεστίου, το οποίο είναι απαραίτητο για τη διατήρηση υγιών οστών. Επιπλέον, η βιταμίνη D συμβάλλει στην ενίσχυση του ανοσοποιητικού μας συστήματος, στην καταπολέμηση των ιών και στην καταπολέμηση της κόπωσης. Έχει συνδεθεί ακόμη και με την καλή διάθεση, με την ανεπάρκεια να οδηγεί ενδεχομένως σε άγχος και κατάθλιψη.
Η βιταμίνη D είναι μια λιποδιαλυτή βιταμίνη που παράγει το σώμα μας όταν το δέρμα εκτίθεται στο ηλιακό φως. Μπορεί επίσης να ληφθεί από ορισμένα τρόφιμα ή συμπληρώματα. Αυτή η βιταμίνη έχει διάφορες μορφές, αλλά οι πιο σημαντικές είναι η βιταμίνη D2 (εργοκαλσιφερόλη) και η βιταμίνη D3 (χοληκαλσιφερόλη). Η βιταμίνη D3 είναι η μορφή που παράγει το δέρμα μας με φυσικό τρόπο ως απάντηση στο ηλιακό φως. Η έρευνα δείχνει ότι τα άτομα με ψωριασική αρθρίτιδα έχουν συχνά χαμηλότερα επίπεδα βιταμίνης D από τους υπόλοιπους (30).
Η λήψη αρκετής βιταμίνης D μπορεί να βοηθήσει στην ανακούφιση ορισμένων συμπτωμάτων ψωριασικής αρθρίτιδας. Ο καλύτερος τρόπος για να εξασφαλιστεί αυτό είναι μέσω της επαρκούς έκθεσης στον ήλιο. Η παραμονή στον ήλιο για περίπου 10 έως 30 λεπτά μεταξύ 10 π.μ. και 3 μ.μ., τουλάχιστον δύο φορές την εβδομάδα, είναι γενικά επαρκής για τα περισσότερα άτομα για την παραγωγή αρκετής βιταμίνης D. Ο ακριβής χρόνος που απαιτείται εξαρτάται από παράγοντες, της ο τύπος του δέρματος, το γεωγραφικό πλάτος, το υψόμετρο και η εποχή.
Το Ιατρικό Συμβούλιο του Εθνικού Ιδρύματος Ψωρίασης συνιστά τη χορήγηση συμπληρώματος βιταμίνης D σε ασθενείς με ψωριασική αρθρίτιδα και ενθάρρυνση στους υπέρβαρους ή παχύσαρκους ασθενείς να διερευνήσουν τη μείωση του βάρους μέσω μιας ελεγχόμενης δίαιτας (31). Ωστόσο, θα πρέπει να ζητήσετε τη συμβουλή του/της ιατρού σας.
Η ενυδάτωση είναι μια άλλη βασική πτυχή που συχνά παραβλέπεται, αλλά είναι ζωτικής σημασίας για τη διαχείριση της ψωριασικής αρθρίτιδας. Αν και δεν υπάρχουν συγκεκριμένες οδηγίες ενυδάτωσης για τα άτομα με ψωριασική αρθρίτιδα, η κατανάλωση περίπου δύο λίτρων νερού καθημερινά, όχι μόνο υποστηρίζει τη διατήρηση της συνολικής υγείας (32), αλλά συμβάλλει επίσης στη λίπανση των αρθρώσεων και στην αποτελεσματική λειτουργία τους, απαλύνοντας τις ενοχλήσεις που σχετίζονται με την κίνηση.
Ορισμένα άτομα διαπιστώνουν ότι συγκεκριμένα τρόφιμα μπορεί να πυροδοτήσουν ή να επιδεινώσουν τα συμπτώματα της ψωριασικής αρθρίτιδας. Αν και οι παράγοντες αυτοί μπορεί να διαφέρουν μεταξύ των ατόμων, οι συνήθεις παράγοντες περιλαμβάνουν το κόκκινο και επεξεργασμένο κρέας, τα χαμηλής ποιότητας λίπη, το αλάτι και τα πρόσθετα, καθώς και τους εξευγενισμένους υδατάνθρακες (Εικόνα 3, δεξιά). Η παρακολούθηση της διατροφής σας και ο εντοπισμός των πιθανών τροφών που πυροδοτούν την ασθένεια μέσω μιας συστηματικής διατροφικής προσέγγισης ή υπό την καθοδήγηση ενός επαγγελματία υγείας μπορεί να βοηθήσει στη διαχείριση του πόνου, της κόπωσης και των εξάρσεων (33).
Είναι σημαντικό να βρείτε καθοδήγηση από έναν πάροχο υγειονομικής περίθαλψης ή έναν διαιτολόγο με εμπειρία στην ψωριασική αρθρίτιδα, για να αναπτύξετε ένα εξατομικευμένο διατροφικό πρόγραμμα (28) ευθυγραμμισμένο με τις ατομικές προτιμήσεις και ανάγκες.
Ένα εξατομικευμένο πλάνο αποσκοπεί στην εξασφάλιση επαρκούς πρόσληψης θρεπτικών συστατικών, στη διαχείριση του βάρους και στην προώθηση της συνολικής ευεξίας, αντιμετωπίζοντας τις μοναδικές προκλήσεις που σχετίζονται με την ψωριασική αρθρίτιδα. Επιπλέον, η υιοθέτηση ενός υγιεινού τρόπου ζωής, που περιλαμβάνει συνεπή σωματική δραστηριότητα, διαχείριση του άγχους και ισορροπημένη διατροφή, ενέχει σημαντικές δυνατότητες βελτίωσης της ποιότητας ζωής των ατόμων με ψωριασική αρθρίτιδα.
Κάπνισμα και κατανάλωση αλκοόλ
Το κάπνισμα είναι κακό για τη συνολική σας υγεία, καθώς αυξάνει την πιθανότητα πιθανών επιπλοκών, όπως καρδιακά προβλήματα και καρκίνο. Το κάπνισμα μπορεί επίσης να σας κάνει λιγότερο ευαίσθητους στη θεραπεία και να επιδεινώσει τα συμπτώματα της ψωρίασης (34, 35).
Το αλκοόλ μπορεί να επηρεάσει την αποτελεσματικότητα ορισμένων φαρμάκων ή να αυξήσει τις παρενέργειες (36, 37). Ορισμένες μελέτες υποδηλώνουν επίσης ότι το αλκοόλ μπορεί να λειτουργήσει ως έναυσμα για τις εξάρσεις (38).